Coronavirus (COVID-19) domestic vaccine certification: equality impact assessment
Equality impact assessment (EQIA) considering positive and negative differential impacts that the domestic Covid Vaccine Certification scheme may have on the nine characteristics protected under the Equality Act 2010.
Title of Proposal: The Health Protection (Coronavirus) (Requirements) (Scotland) Amendment (No. 2) Regulations 2021
Legislative Background
The Health Protection (Coronavirus) (Requirements) (Scotland) Amendment (No. 2) Regulations 2021 (the 'Regulations') are made under powers to make provision for the purpose of preventing, protecting against, controlling or providing a public health response to the incidence or spread of infection, conferred on the Scottish Ministers by schedule 19 of the Coronavirus Act 2020. They amend the Health Protection (Coronavirus) (Requirements) (Scotland) Regulations 2021 (the 'Principal Regulations').
Introduction
The aim of this Equality Impact Assessment (EQIA) is to analyse the potential impacts for each protected characteristic under the Equality Act 2010, both positive and negative, of using Covid Vaccine Certification domestically. Where there are potential negative impacts, mitigating actions have been identified. The use of Covid Vaccine Certification for international travel is beyond the scope of this impact assessment, and a separate EQIA on this policy can be found online.
The Scottish Government is mindful of the three aims of the Public Sector Equality Duty (PSED): eliminate unlawful discrimination, harassment and victimisation; advance equality of opportunity between people who share a protected characteristic and those who do not; and foster good relations between people who share a protected characteristic and those who do not[1]. We are also mindful that the equality duty is not just about negating or mitigating negative impacts as we also have a positive duty to promote equality, and so we have therefore sought to promote equality through both the policy itself and support and guidance.
While it is the view of the Scottish Government that any remaining impacts of Covid Vaccine Certification are currently justified, and a proportionate means of helping to achieve the goals set out in the Policy Objectives section, we also recognise that these measures are only required to respond to the current set of circumstances, and are only necessary as long as the potential public health benefits can justify any negative impacts caused.
International evidence suggests that crises responses often inadvertently discriminate. The Equality and Human Rights Commission, the Scottish Human Rights Commission and the Children's Commissioner for Scotland stated in April 2020 they had already found increasing evidence that some groups are experiencing disproportionately negative impacts from the virus and some of the responses to it.[2]
The Scottish Government are committed to ensuring that human rights, children's rights and equality are embedded in everything we do, and are central to our response to the pandemic. The Scottish Government's Framework for Decision Making recognises that harms caused by the pandemic do not impact everyone equally, and that we must work to advance equality and protect human rights.
Policy proposal
Covid Vaccine Certification will require certain premises and settings to ensure that there a reasonable system in operation for establishing that all people in the premises can demonstrate that they are fully vaccinated (or "possess Certification", unless they fall into one of the exempt categories), and to refuse access to or remove anyone who is neither fully vaccinated or exempt. "Fully vaccinated" means that a person has completed a full course of an authorised vaccine, with the final dose having been received 14 days before the date on which they seek to enter the premises or event.
Initially, the scheme will not include a negative test result as an alternative to proof of vaccination, but this will be kept under review. At this stage, we do not consider that including testing results would be appropriate, and believe it could undermine one of the policy aims of the scheme: to increase vaccine uptake. Also, it is important at this stage to prioritise PCR lab capacity for Test and Protect purposes. While promoting regular lateral flow tests (LFD) tests is an extremely important aspect of our overall approach, further work would be required on an optimal approach to incorporating testing into Certification, including consideration of the appropriateness of self-testing in this context.
Furthermore, the scheme will apply in the following higher risk settings:
- late night premises with music, which serve alcohol after midnight and have a designated place for dancing for customers
- indoor events (unseated) planned for 500 or more people at any one time
- outdoor events (unseated) planned for 4,000 or more people at any one time
- any event planned for more than 10,000 people at any one time
The following will not qualify as events for the purposes of the scheme:
- a funeral, marriage ceremony, civil partnership registration, or a reception or gathering which relates to a funeral, marriage ceremony or civil partnership registration
- a mass participation event such as a marathon, triathlon or charity walk
- an event designated by the Scottish Ministers as a flagship event according to criteria, and in a list published by the Scottish Ministers
- a showing in a cinema
- a drive-in event
- an organised picket
- a public or street market
- an illuminated trail
- a work or business conference (not including any peripheral reception or function outside the core hours of the conference, whether or not alcohol is served)
- a business or trade event which is not open to the public for leisure purposes
- communal religious worship
- an un-ticketed event held at an outdoor public place with no fixed entry points
Trade events attended by members of the public for leisure purposes, for example wedding fairs and craft fairs would not be excepted. The people working at the event (such as exhibitors and venue staff) would be excepted.
Ministers have been clear that certification will not be a requirement for public services or other settings that many people have no option but to attend, such as retail, public transport, health services and education.
The following people will be exempt:
- under 18s
- people who cannot be vaccinated for medical reasons
- people taking part (or who have taken part) in vaccine trials
- the person responsible for the premises
- workers and volunteers at the premises or event
- emergency services responders and regulators carrying out their work
The regulations will require the persons responsible for late night premises or a relevant event to ensure there is a reasonable system in operation for checking that people seeking to enter the premises are fully vaccinated or are exempt, and to have in place a compliance plan for the system.
The scheme will come into force at 5 am on 1 October 2021. The requirement on persons responsible for late night premises or a relevant event to ensure there is a reasonable system in operation for checking Certification will not be enforceable under Part 4 of Health Protection (Coronavirus) (Requirements) (Scotland) Regulations 2021 until 18 October 2021.
The requirement to have a compliance plan applies from 5 am on 18 October 2021.
Ministers must review the Health Protection (Coronavirus) (Requirements) (Scotland) Regulations 2021 (which include Certification) at least every 3 weeks to assess whether any requirement in the regulations is still necessary to prevent, protect against or provide a public health response to the incidence or spread of infection in Scotland. We will continue to assess whether any less intrusive measures could be introduced to achieve the same combination of policy objectives in respect of the higher risk sectors concerned; if so, the policy will be immediately reviewed.
Sectoral Guidance is published on the Scottish Government website.
Guidance for the wider public has been published on the Scottish Government website.
Policy Objectives
In line with our strategic intent to 'suppress the virus to a level consistent with alleviating its harms while we recover and rebuild for a better future', the policy objectives of Covid Vaccine Certification are to:
- reduce the risk of transmission of Coronavirus
- reduce the risk of serious illness and death thereby alleviating current and future pressure on the National Health Service
- allow higher risk settings to continue to operate as an alternative to closure or more restrictive measures
- increase vaccine uptake
An evidence paper summarising the range of evidence available on Vaccine Certification schemes has been published alongside the impact assessments. Consistent with our approach throughout the pandemic, the paper adopts a four harms approach covering the direct health harms of Covid-19, the indirect health harms, the social and the economic harms. Evidence is drawn from clinical and scientific literature, from public opinion and from international experience.
Public Health rationale
Although daily Covid case numbers are dropping in Scotland, case numbers remain too high, and we still have a large susceptible population which could lead to cases rising again. In addition, the number of people in hospital and ICU continues to increase. The winter period ahead will pose significant challenges of increased transmission and related pressure on the National Health Service—this impact assessment should be considered alongside the latest State of the Epidemic report. We remain of the view that action is therefore needed across all sectors to ensure adherence to baseline measures. Drawing on the evidence so far available, we consider that Vaccine Certification has a vital role to play as one such measure.
While no vaccine is 100% effective at preventing infection, disease and transmission, and they do not completely break the link between a high volume of positive cases and serious pressure on healthcare services, they are our best route out of the pandemic. Vaccines help prevent transmission of the virus as vaccinated people are less likely to become infected and ill than unvaccinated people (and only infected people can transmit the virus). The UK Vaccine Effectiveness Expert Panel (VEEP) is a group of scientific and analytical specialists from academia and government in the UK who provide a consensus view on vaccine effectiveness, split by variant, vaccine and dose. They have published estimates for vaccine effectiveness based on an assessment of the evidence at the time of writing and as new evidence or data emerges, SAGE will update its advice. A summary published on 27th August can be found online.
More analysis can be found in a number of large studies including EAVE-II (Early Pandemic Evaluation and Enhanced Surveillance of Covid-19) in Scotland[3], Real-time Assessment of Community Transmission (REACT-1) in England[4] and the Office for National Statistics (ONS) Covid-19 Infection Survey ONS study.[5] Therefore, we have strong evidence that vaccines are effective at preventing disease, hospitalisations and deaths: in the four weeks from 21 August 2021 to 17 September 2021, Covid-19 cases increased and surpassed the peak that was seen in early July. Although case rates are now declining, the rate of increase in cases then was less among fully vaccinated individuals: As of 29 September, 70.0% of the population were fully vaccinated, and in the week 18-24 September 46.9% of positive cases were in unvaccinated individuals. However, effectiveness decreases over time for both Pfizer-BioNTech and Oxford-AstraZeneca vaccines due to waning immunity.[6]
High-risk settings tend to have the following characteristics: close proximity with people from other households; settings where individuals stay for prolonged periods of time; high frequency of contacts; confined shared environments, and poor ventilation.[78] Therefore, by restricting access in these settings to customers who are fully vaccinated, these are less likely to be settings of infection, and it is less likely that infections within them will lead to illness. Consequently, we can reduce the risk of transmission of the virus and help reduce pressure on health services while also allowing settings to operate as an alternative to closure or more restrictive measures. As such, we consider Certification, as part of a package of measures such as improved ventilation, to be a necessary and proportionate public health measure.
NHS Scotland Covid App and Paper Certificate
On 30 September we will launch the NHS Scotland Covid Status App, which contains 2 Unique QR codes, with the first detailing a person's name, date of birth and first vaccination, and the second just holding data on their 2nd vaccination. Further information, such as testing status or recovery status, will be added in a future release of the App. The Privacy Notice is already online and can be found on NHS Inform: Personal information we process, How we use your data, Your Rights. The Easy Read Version can be found online. This product has been designed for use for international travel and so it is necessary to include these details to meet EU standards. This App can be used to demonstrate vaccine status in the regulated settings.
A domestic version of the App is expected to launch in mid-October. This will simply show the person's name and whether they have Certification, demonstrated as either a green tick or red cross through the use of the NHS Scotland Covid Check App. The domestic App will have functionality to hide and display a person's name.
For those who do not have digital access or would prefer a paper copy, a record of vaccination can be requested by phoning the Covid-19 Status Helpline on 0808 196 8565. The paper record of vaccination will then be posted to the address that is held on the National Vaccination Service System (NVSS).
When registering an account on the App the user needs to verify their identity. This is for privacy protection, to ensure that the user's identity has been verified before they are given access to medical records.
The App will use biometric identification software at the set up stage. This means users will be asked to scan a photo of their ID – for example a passport or driving license – and then take a live photo or video of themselves. The software will then use their live photo to compare likeness with the photo in their ID and confirm their identity. There will be manual verification for the small number of cases which fail the automatic process. For the limited number of cases where a person's identity cannot be verified in the App or through manual intervention, the individual can call the Covid-19 Status Helpline or use NHS Inform to request a paper Certificate, which will be posted to them.
Individuals who are medically exempt can apply for a paper Certificate through the NHS Inform website. This will be a paper Certificate and will have enhanced security features. Medical exemptions cannot be displayed on the international App due to EU specification but may be included in a future release of the domestic App.
All clinical trial participants have received a letter from their Principal Investigator which can be used for proof of their trial status and to access a regulated setting. All Clinical Trial Participants have already received a secure Certificate indicating their trial status. This enables people to gain access to domestic venues where Certification is required.
While children are exempt from the requirement to prove Certification for domestic purposes, 12-17 year olds who have been vaccinated may choose to download a PDF via NHS Inform, or they may choose to request a paper Certificate by calling the Covid-19 Status Helpline.
We are translating documents explaining what is shown on your Certificate into different languages and developing an Easy Read, Braille and large print version of the paper Certificate. There will also be available in audio format and British Sign Language. These will be available in the future.
For more information on the Covid Vaccine Certificate see the Scottish Government website.
Age: Young people (18-39)
Background
A full Children's Rights and Wellbeing Impact Assessment (CRWIA) on the use of Vaccine Certification for international travel has been carried out and can be found on the Legislation.gov.uk website. The CRWIA considers the impact of Certification on children – all those under 18 – and so this age group will not be considered in the EQIA.
Young people in the age cohort 18-39 have taken up vaccination at lower rates than the rest of the population. As of 20 September 2021, 76% of young adults aged 18-29 had received one dose, with 61.7% being fully vaccinated; 83.2% of adults aged 30-39 had received one dose, with 74% being fully vaccinated.[9] UK-wide research suggests that, while general willingness to get vaccinated is high, vaccine hesitancy (the "reluctance or refusal to vaccinate despite the availability of vaccines"[10]) is inversely related to age, as 16–24 year olds are 1.48 more likely to be vaccine hesitant than those aged 45–54 years.[11]
Connected with this lower vaccination uptake among younger cohorts, Public Health Scotland data shows that, in the four weeks up to 30 August 2021, 40.1% of Covid-19 related acute hospital admissions were unvaccinated individuals, of which 56.2% were in the under-40s age group.[12]
Even before the pandemic, young people already reported higher levels of loneliness than the general population. The Scottish Household Survey of 2018 showed that 21% of the general population reported feeling lonely "some, most, almost all or all of the time" in the last week, but this percentage rose to 24% for people aged 16-24.[13] During the pandemic, evidence suggests that young people's mental health has suffered disproportionately from restrictions. In the first wave, 18-29 year-olds reported 1.7 times more depression, 1.6 times more anxiety, and almost twice as many suicidal thoughts than the overall sample.[14] In the second wave, levels of anxiety for that age group increased further.[15]
Differential impacts
Positive Impacts
This age cohort (18-39) have the lowest level of vaccination. The date of 1 October was selected as an appropriate implementation date as by this point all over 18s will have had the opportunity to be fully vaccinated and two weeks, the time taken for the vaccine to take effect, will have passed. If the policy objective is achieved and vaccine uptake increases among this age group then it would positively impact them as it would reduce their direct health harms from Covid-19.
All 16 and 17 year olds were invited to come forward for vaccination from 6 August.[16] 17 year olds who are turning 18 when certification comes into force, who have not had time to be fully vaccinated, will be covered by the exemption for under 18s.
Socialisation is key in supporting and maintaining relationships, mental health and wellbeing. Evidence shows that the mental health of this age group declined during lockdowns, and then gradually increased as settings re-opened.[17] [18] The settings in scope are often frequented by young people and play an important role in facilitating socialisation. Therefore, if the policy objective is achieved and the risk of transmission is reduced, which in turn allows higher risk settings to continue to operate as an alternative to closure or more restrictive measures, the policy could positively impact young people as it facilitates their ability to socialise.
Negative Impacts
There are some young people, such as some care experienced people, who may find it more challenging to access and maintain Certification due to their life experiences and circumstances. For example, a care experienced person may change their address frequently, and may not have their current address registered at their GP.
There is a possibility that Certification could be used beyond the intended purposes, and that employers could require proof of vaccination as a condition of employment. Employees within the regulated settings are generally younger: evidence from the Institute for Fiscal Studies showed that young people (under 25s) in the UK were 2.5 times as likely to work in a sector that has been 'shut down' during the pandemic, such as leisure and entertainment.[19] Therefore, if employers within scope use Certification beyond the policy intention, it is more likely to impact on younger people. This age group has been already impacted financially by the pandemic, so if people are not able to maintain or gain employment due to lacking vaccination status this may exacerbate pre-existing challenges.
Age: Older People
Background
Older people have been particularly impacted by the health harms of the virus. Up to 19 September 2021, there were 13% excess deaths in people aged 85 or older, with excess deaths in people aged 75-84 at 12% above average. Most of these excess deaths occurred at the beginning of the pandemic in April 2020.[20] Up to March 2021, the death rate involving Covid-19 for people over 70 was more than six times the death rate for those aged 40-65.[21]
Prior to the pandemic, older people suffered disproportionately from feeling lonely. The Scottish Household Survey of 2018 showed that 21% of the general population reported feeling lonely "some, most, almost all or all of the time" in the last week. The percentage rose to 25% for people aged 75 and over.[22]
Social isolation and loneliness has been exacerbated by Covid restrictions and a key group affected are those aged over 75. A report from Age UK suggests that the pandemic has had a damaging effect on older people's mental health: 34% of those surveyed agreed that their anxiety was worse or much worse than before the start of the pandemic. Of those surveyed aged over 70, 31% reported feeling unsafe or very unsafe, and 45% uncomfortable or very uncomfortable when outside of their home due to the pandemic.[23]
There have been significant wider impacts on older people. In March 2020, about 180,000 individuals (3% of the Scottish population) who were clinically extremely vulnerable (CEV) were asked to shield. CEV individuals are more likely to be female, older, and live in more deprived areas of Scotland than the population at large.[24] A study on the experience of those shielding found that 87% reported a negative impact to their quality of life, 85% a negative impact on physical activity and 72% a negative impact on their mental health.[25]
Differential impacts
Positive impacts
If the policy objectives to reduce the risk of transmission and to increase vaccine uptake are achieved this would positively impact older people, as any reduction in transmission of the virus will positively impact this group who are at a far higher risk of poorer health outcomes if they contract the virus.
Age Scotland suggested that Certification could play a positive role in supporting older people to feel safer and more confident in society if they know that those around them are vaccinated. This is particularly the case for those older people who are clinically extremely vulnerable.
Lockdowns and restrictions have negatively impacted older people's mental health and wellbeing. If the policy objective is achieved and higher risk settings can to continue to operate as an alternative to closure or more restrictive measures, this could positively impact older people if, for example, they are still able to attend the settings in scope with family, friends and support groups and services.
Negative impacts
Digital access reduces with age. As of 2019, 20% of over-55s in the UK do not own a smartphone[26] and only 47% of adults aged 75+ use a smartphone to access the internet, compared to 98% of 16-24 year olds.[27] Certification will therefore be available both digitally (via an App) and as a paper document. Stakeholders have highlighted that although paper Certification would mitigate against digital exclusion, it may still present challenges depending on how easy it is to update (for instance if data is incorrect or out of date) and on what happens when a Certificate is lost, stolen or destroyed.
When registering on the App for the first time, the user needs to verify their identity before they can access their health records. This will done using biometric identity verification: a facial recognition software which will compare the photo in a person's ID with a live photo or video.
Stakeholders raised this as a potential issue, as some older people have never had ID, or it has expired and not been renewed. Stakeholders cited research commissioned by the Cabinet Office for the introduction of mandatory photo ID at polling stations, which suggests that 2% of people aged over 70 in Great Britain do not have any form of ID.[28]
However, those who cannot verify their identity on the App can call the free national helpline and request a paper copy of their Certification, or use the Covid Vaccination and Scheduling Portal. The Covid-19 Status Helpline is free and open every day from 10:00-18:00. A Resolver Group has also been established to resolve any reported inaccuracies in vaccination records and wider issues relating to acquiring Covid Vaccination Certification. We are translating documents explaining what is shown on your Certificate into different languages, and developing Easy Read, Braille, and large print versions of the paper Certificate, which will also be available in audio format and British Sign Language. These will be available in the future.
As a vaccine certificate will be required to access some settings, it could potentially be used as a method of coercive control, for example by taking a phone or paper certificate from the victim. Although older people have historically been a 'hidden' group in domestic abuse statistics, UK research from 2016 suggests that victims aged 61+ are much more likely to experience abuse from a family member, much more likely to suffer abuse from a current intimate partner and more likely to keep living with the perpetrator after getting support.[29]
Lastly, some older people rely on carers and others, including family members, for everyday living. If someone who cares for an older person does not have Certification, this could negatively impact on the older person if they are not able to access the setting in scope due to not having support from their carer.
Disability
Background
According to the 2019 Scottish Health Survey, 32% of men and 37% of women in Scotland reported living with a limiting long-term condition. For people aged 75 and over, 58% had a limiting long-term condition.[30] 1 in 5 Scots identify as disabled, and more than a quarter of working age people have an acquired impairment.[31]
Covid has had a disproportionate impact on the health of disabled people: 93% of people who died from Covid-19 up until April 2021 had at least one pre-existing condition.[32] Research by National Records of Scotland with deaths data until January 2021 found that, after adjusting for age, disabled people were between 1.8 to 3.2 (women) and 1.8 to 3 (men) times more likely to die with Covid-19 than non-disabled people, depending on the extent to which disability limited their daily activities.[33] Similarly, research in England which analysed data from up to February 2021 estimated that, after adjusting for age, sex, ethnicity, and geographical location, adults on the learning disability register were 5.3 times more likely to be hospitalised in relation to Covid-19, and 8.2 times more likely to die due to Covid-19.[34]
Covid-19 restrictions have impacted disabled people particularly hard. Evidence has highlighted how, for wheelchair users, their main option to meet others was indoors, whilst others with dementia or learning disabilities struggled to understand the rapidly changing restrictions.[35] Other evidence suggests that people with pre-existing mental or physical conditions feel negatively affected by the fact that others seem to now be living more normally than they do, and those with physical health conditions are among the sub-groups with the highest level of concern about the occurrence of another wave of Covid-19.[15]
Differential impacts
Positive impacts
If the policy objectives to reduce the risk of transmission and to increase vaccine uptake are achieved, this would positively impact those disabled people who are at a far higher risk of poorer health outcomes if they contract the virus.
Some disabled people who are clinically extremely vulnerable were asked to shield at the start of the pandemic. Anecdotal evidence suggests that while shielding officially ended on 26 April 2021, concerns about contracting the virus have remained, and many individuals have continued to behave as if they are still shielding, leading to an adverse impact on their lives and quality of life. Certification could provide reassurance for these people and support them to feel safer and more confident in society.
Additionally, if the policy objective to allow higher risk settings to continue to operate as an alternative to closure or more restrictive measures is achieved, Certification could benefit disabled people as socialisation plays a key role in disabled people's wellbeing. Therefore, if Certification supports settings to remain open and facilitates socialisation—such as the ability to attending the settings in scope with family, friends and support groups and services—this would lead to positive impacts for disabled people.
Negative impacts
As with age, digital exclusion is a key consideration for disabled people. Glasgow Disability Alliance reports that 60% of their members feel digitally excluded[36] and that, while disabled people may have a smartphone, it may be too old to support certain Apps.[37] [38] Some disabled people may use an older model of mobile phone if it meets their accessibility needs.
As with many other products which are part of everyday life, such as bus passes, there may be limited circumstances where a disabled person finds it challenging to maintain either a digital or paper Certificate. According to the latest statistics, in 2019 there were 23,584 adults in the autistic spectrum or with learning disabilities known to local authorities in Scotland.[39] Some of these people may find it more challenging to maintain Certification, which could lead to negative impacts if it results in them not being able to access a setting in scope. They may also find the experience of being turned away confusing and distressing. In these circumstances, an individual or their carer or other relevant adult can call the Covid-19 Status Helpline and request a paper copy of Certification on behalf of the person they are caring for.
There are exemptions in the regulations for the very small percentage of the population who cannot be vaccinated for medical reasons. Some people who are exempt from vaccination may have a condition which would be considered a disability under the Equality Act.[40]
While the details of a person's exemption will not be displayed on their exemption Certificate – it will simply say 'Exempt' – stakeholders have nonetheless raised concerns about data protection, as health data is special category data and protected under human rights legislation (Article 8 right to respect for private and family life). Stakeholders have also raised concerns that, for the very small proportion of disabled people who are exempt, some will be denied access to the regulated settings, even though they have an exemption, as has been experienced with face covering exemptions. Medical exemptions cannot be displayed on the international App due to EU specification, but may be available in a future iteration of the App which would not show medical data to a person who scans an exempt person's Certificate.
Stakeholders also highlighted that disabled people are more at risk of becoming victims of a variety of scams, and this is substantiated by an information briefing from Citizens Advice in June 2018.[41] Certification may then provide "phishing" opportunities for scammers, which may impact disabled people more than non-disabled people.
Certification may negatively impact disabled people if their carer has a different status to themselves. Data from England shows that 91% of carers known to local authorities care for someone with a physical disability or a long-standing illness[42] and 31.3% of Scottish adults with a learning disability live with a family carer.
As with older people, there is the potential for a Covid vaccine certificate to be used as a tool to exert coercive control. A report from Public Health England in 2015 indicated that disabled people experience higher rates of domestic abuse and suffer it for longer periods of time, more severely and more frequently.[43] Data from Glasgow over 2018-20 shows that 12% and 22% of Adult Support and Protection investigations involved someone with a physical or a learning disability, respectively.[44]
Gender Re-assignment
Background
As of May 2018, around 0.5% of the population of Scotland (24,000 people) were estimated to be transgender.[45]
Trans people suffer disproportionately from mental health conditions. A systematic review concluded that they were twice as likely as the general population to take their own lives and that a lack of access to health care places particular pressure on trans communities.[46] A 2020 review of literature on trans people and loneliness found that trans people often report higher levels of loneliness than the general population. It also found that belonging to communities of people who face similar challenges has a positive psychological impact on trans people's wellbeing.[47]
Differential impacts
Positive impacts
Socialisation is important for many trans people and is essential in maintaining their mental health and wellbeing. Therefore, if the policy objective is achieved and the risk of transmission is reduced, which in turn allows higher risk settings to continue to operate as an alternative to closure or more restrictive measures, Certification could positively impact trans people as it supports their ability to socialise.
Negative impacts
Many trans people may be known by different names, pronouns, and genders by different people, institutions, and databases at various points in their lives. If changes have not carried across all data sets, people may have different names and genders on different healthcare databases, which stakeholders have advised can cause data flow and interoperability issues. Stakeholders have also informed us that in a few circumstances entire health care records have been deleted and a new profile created when an individual has asked for their name or gender to be changed.
When registering on the App for the first time, the user needs to verify their identity before they can access their health records. This will done using biometric identity verification in the form of facial recognition software which will compare the photo in a person's ID with a live photo or video. Then, the details on the ID are used to match the user to their health record.
This presents a number of practical problems for trans people. Firstly, we know that LGBT people are less likely to have valid ID and may therefore find it more difficult to verify their identity on the App. Cabinet Office research found that 96% of gay and lesbian respondents own at least one form of photo ID, compared to 98% of heterosexual respondents.28[28] Unpublished interim findings from a joint survey run by Stonewall and LGBT Foundation found that: nearly one in four respondents (23%) had experienced problems having ID accepted in the past; just under three quarters of respondents (73%) owned a usable UK passport, and just over two thirds of respondents (68%) owned a usable driving license ('usable' = where the photo looks like them and the personal data matches their name and gender. Out of date ID is still 'usable' for the purposes of the survey). The top five most common barriers or concerns cited in relation to obtaining ID were: receiving intrusive questions from other people when applying for or presenting ID (38%); obtaining ID taking more energy than they have available (37%); being unable to easily print documents (32%); being 'outed' as trans when applying for or presenting ID (31%) and obtaining ID taking more time than they have available (26%). For those who have no ID and are therefore unable to register with the App, they will still have access to the paper alternative, as this can be posted to the address held on health databases.
If they do have ID, trans people may then encounter other issues relating to the verification process. The biometric identification software will compare the photo on the ID with a real time photo or video of the individual. For some trans people their photo could look different to their current appearance for a number of reasons, including that they are wearing make-up, they have taken hormones or undergone facial surgery. This may mean that the software is not able to automatically verify the person's identify. Gender and racial biases within facial recognition software are known in the technology industry ,and stakeholders highlighted that minority ethnic (ME) communities and trans people often have lower rates of automatic verification with this type of software, and stated that this could be particularly true for trans ME people.[48] Jumio, the company providing the software, works to minimise demographic bias in their AI algorithms by using large and representative data sets and training its AI on real-word production data.
After the biometric verification check, a last barrier for trans people is that if the individual's details on their ID differ from those on their medical records, they might not be able to register their account. Stakeholders have informed us that trans people often have turbulent interactions and relationships with health care services, so if Certification creates the need for increased interactions of this kind then it could potentially cause additional anxiety and distress.
Once an account has been created, stakeholders have highlighted the risk that Certification could lead to discrimination and distress if a user's name is displayed on the App or certificate. For example, if someone's name on their medical records – and therefore their certificate – is different to the name that they use with their friends, family and others, this could lead to their transgender identity being unintentionally disclosed. The domestic App will have functionality to hide and display a person's name. Individuals can create separate profiles for international and domestic use using different email addresses. If an individual wishes to use a different name domestically, and has photo ID in that name, they can create one account for international travel, which aligns with the details on their passport, and one account for domestic use, which aligns with their preferred name.
If a trans person cannot verify their identity on the App, requests a paper Certificate, and the document is posted to their family home, this could unintentionally reveal their trans status to family members. LGBT young people are already fearful of disclosing their identity – 'coming out' – and 77% of young people believed their sexual/gender identity was a causal factor in their rejection from home.[49]
Marriage & Civil Partnership[1]
Background
During the pandemic there has been a reduction in the number of new marriages and civil partnerships: there were 5,545 marriages registered in Scotland between 1 April and 30 June 2021, 30% lower than the average number on a second quarter over the five years 2015-19, but a large increase on the number of marriages in the same period in 2020 following the easing of Covid-19 restrictions.[50] This was mainly due to the fact that Registration Offices closed mid-March and most marriages scheduled after the closure could not take place. From June 2020 onwards marriages and civil partnerships were resumed but with very strict limits on the number of attendees.
UK polling data gives us further indications of the extent to which couples who wanted to get married or registered as a civil partnership have been impacted by the pandemic. A poll of more than 400 couples with weddings planned between September 2020 and January 2021 revealed that, while 95% are not planning to cancel their wedding, 71% were choosing to postpone to later in the year or into 2022.[51] This is corroborated by a survey of 1,449 people who had planned to marry during the first lockdown in summer 2020 in England and Wales: 625 (43%) of respondents had been unable to marry on their intended wedding date, with the majority of them having to postpone their plans.[52] More recent YouGov polling data from June 2021, which covered more than 3,200 adults in Great Britain, reveals that 91% of respondents have not attended a wedding in the last year or so, under Covid-19 restrictions. Of the very small number of respondents who have (6%), half of them (3%) said that the experience had not been as good as it could have been without Covid-19 restrictions.[53]
Differential impacts
Positive impacts
There is an exception for funerals, marriage ceremonies or civil partnerships and related post ceremony gatherings from the requirement for Certification.
Negative impacts
If partners or spouses have differing Certification status then this could potentially have negative impacts if one person is not able to enter a setting in scope while the other is.
Pregnancy and Maternity
Background
Current evidence suggests that pregnant women are no more likely to get Covid-19 than adults without health conditions, but that they may be at increased risk of becoming severely unwell compared to women who are not pregnant, particularly in the third trimester.[54]
A study from the American Journal of Obstetrics and Gynaecology that studied more than 340,000 births in England up to January 2021 found that women who tested positive for Covid-19 around the time of birth were twice as likely to have a stillbirth, and were more likely to have an emergency caesarean birth compared with those who didn't have Covid-19 when giving birth. Another global study of 2,100 pregnant women across 18 countries found that women who contracted Covid-19 during pregnancy were over 50% more likely to experience pregnancy complications, and that their risk of dying during pregnancy and in the postnatal period was 22 times higher than in the non-infected pregnant women.[55] Although there was less evidence earlier in the pandemic, pregnant women had been included in the list of people at moderate risk if they contracted the virus as a precaution, and a small number were asked to shield during the pandemic if they had congenital or acquired heart disease.[56]
The virus has also impacted pregnant women's wellbeing and economic prospects. A survey of almost 20,000 mothers and pregnant women, conducted after the first wave by Pregnant Then Screwed, showed that 15% of mothers surveyed were either made redundant or expected to be made redundant. 72% of mothers reported needing to work fewer hours because of childcare issues, and 65% of mothers who were furloughed said a lack of childcare was the reason.[57]
Differential impacts
Positive impacts
Public insights polling has found that 53% of those surveyed agreed that the high level of people with two doses of the vaccine in Scotland gives them more confidence to go out and about[58] and 62% of respondents agreed that, it they wanted to go to premises or an event, having a Covid Vaccine Certification scheme in place would make them feel more comfortable doing this.[59] This was particularly true of women, who were 7 percentage points more likely to agree that it would make them feel more comfortable (women 65% vs men 58%).
Therefore Certification could add a layer of reassurance to pregnant women and support them to feel safer and more confident participating in society: more recent polling of 9,000 pregnant women by Pregnant Then Screwed showed that three quarters of respondents said they feel anxious about the easing of Covid-19 restrictions.[60]
Stakeholders highlighted that, if the policy objective to allow higher risk settings continue to operate as an alternative to closure or more restrictive measures is achieved, Certification would be welcomed by many pregnant women as they have been negatively and sharply impacted by the economic burden of restrictions and lockdowns.
Negative impacts
We know that vaccine hesitancy is higher in women, particularly younger women, in part due to fears related to fertility.[61] Stakeholders have highlighted anecdotal evidence that women who conceived through IVF are particularly vaccine hesitant. Whilst direct comparisons are not currently available, the data on Covid-19 vaccination in pregnancy shows that, to date, vaccination rates have been lower in pregnant women compared to non-pregnant women in the same age groups. Public Health Scotland data shows that 30% of women aged 35-39 who delivered their baby in July 2021 had received a Covid-19 vaccination by the time of delivery. By contrast, data available for the general population shows that by the end of July 2021, 81% of adults aged 30-39 years in the general population had received a vaccine.[62] Pregnant women would could therefore be impacted by Certification if they are not vaccinated and are denied access to the settings in scope.
There are very few circumstances where pregnant women are advised against vaccination due to pregnancy related complications. In these circumstances, they will be eligible to apply for an exemption on the NHS Inform website. If Certification exceeds the policy intention and is used by private businesses or third parties as a condition or employment, then this could negatively impact on pregnant women if they have not been vaccinated. Businesses which are not covered by the Government's scheme are required to meet their obligations under all relevant law including data protection, the Equality Act and Human rights. For more information see the Equality and Human Rights Commission Guidance for Employers.
Race
Background
Minority ethnic people in Scotland experience significant health inequalities. Prevalence of some health conditions are higher for some ethnic groups, such as Type 2 diabetes and coronary heart/cardiovascular disease among people of South Asian and African descent. In 2011, despite having a much younger age profile, 37% of Gypsy/Travellers reported having long-term health conditions compared to 30% of the population as a whole.[63]
Inequalities are also socioeconomic. Relative poverty, which affected 23% of households in Scotland in 2019, rose to 38% and 39% in Black and Asian households respectively.[64] The gap in employment rates for working age minority ethnic people, relative to the white population, was 22% for women and 9.5% in men, and Pakistani and Bangladeshi workers had the lowest median hourly pay and were also the least likely to work from home in the UK.[65]
The pandemic has exacerbated existing health and wider inequalities. Scottish research has shown that rates of hospitalisation or death from Covid-19 were three times higher in Pakistani and Mixed groups, and around two times higher in Indian and Other Asian groups than the white population.[66] Estimates show that low earners were 7 times more likely than high earners to have worked in a sector that has shut down as a result of the lockdown, and those with customer facing roles are likely to have seen reductions in earnings or face job losses as they are less able to work from home.[67]
Differential impacts
Positive impacts
If the policy objectives to reduce the risk of transmission and to increase vaccine uptake are achieved, Certification could benefit minority ethnic communities, as they are at a higher risk of poorer health outcomes if they contract the virus.
A panel study with more than 70,000 participants across the UK undertaken by University College London suggests that minority ethnic people describe higher levels of loneliness than their White counterparts.[68] Therefore, if the policy objective to allow higher risk settings to continue to operate as an alternative to closure or more restrictive measures is achieved, Certification could benefit minority ethnic groups by facilitating socialisation.
Negative impacts
People from certain ethnicities, for many different reasons, are less inclined to take up the vaccine. Low uptake is a result of a combination of factors including misinformation, mistrust, socioeconomic barriers, and delivery that does not meet accessibility needs. For example, some Gypsy/Travellers are often not in an area long enough to engage with health services to receive both vaccinations.
Looking at ethnicity, the uptake of the first dose by most ethnic groups is lower than the White group for all age cohorts.

Source: Public Health Scotland
Survey data from UK-wide research suggests that, in comparison to White British and White Irish participants, Black African and Mixed Black African health and social care workers were less likely to have been offered a vaccine, and much more likely to have declined vaccination if offered. Reasons for doing so among Black African participants included distrust in Covid-19 vaccinations, healthcare providers and policymakers.[69] Uptake by the White Polish community is also comparatively much lower.[70] Therefore Certification could negatively impact ME communities if they are denied access to the regulated settings due as they have not been vaccinated.
Stakeholders raised concerns that the introduction of Certification could exacerbate vaccine hesitancy and thus undermine one of our policy objectives. They felt that Certification is unlikely to incentivise asylum seekers, refugees or migrants to take up the vaccine as they do not often frequent the settings in scope. Stakeholders also felt that as parents and guardians are influential figures in children's lives, children may hold the same sentiments as their parents, and may also become less likely to take up the vaccine.
Certification could also impact migrants. Research suggests that the majority of documented migrants that are recent entrants to the UK do not register with a GP, despite relatively easy access to primary healthcare.[71] Undocumented migrants, refugees and asylum seekers are even less likely to register in primary care services.[72] Stakeholders identified that a reason for this is fear that their data will be shared with the Home Office, which could impact on their migration status. This is based on prior experience of health data being shared by the NHS with the Home Office, which resulted in deportations.[7374]
We know people from lower socio-economic backgrounds are more likely to be digitally excluded. For example, 82% of households in the 20% most deprived areas in Scotland had internet access at home compared with 96% of households in the 20% least deprived areas.[75] We also know that relative poverty impacts ME people far more than White people and so minority ethnic communities are more likely to be digitally excluded. Paper certificates are available as an alternative, together with support and guidance. Whilst this is a sound option, it may still present some challenges. For example, as a security measure, the paper Certificate is posted to the address held by the GP. This could impact some groups, such as some Gypsy/Travellers, who may not have a fixed address.
In terms of the App, as previously explained under the Gender Reassignment section, facial recognition software has been found to contain racial and gender biases. This may mean that a higher number of minority ethnic people, especially women, registering for the App could encounter more difficulties verifying their identity than white people.[76] Stakeholders also highlighted that migrants, asylum seekers and refugees, are less likely to have ID, and as such may be unable to use the App.
There is also the possibility that Certification could be used beyond the intended purposes and employers could require proof of vaccination as a condition of employment. People from ethnic minorities are disproportionately represented in industries where working from home is not feasible, and may therefore be more impacted if employers enforce this requirement.[63] This is particularly true as they are less likely to have taken up the vaccine than their white colleagues.
As with anything where documentation affords access to certain spaces, services or products, there is the potential that unconscious bias could cause enforcement of Covid Vaccine Certificate to be administered in a discriminatory manner. There are more subtle ways that unconscious bias could be enacted, as for example while taking all reasonable measures to enforce Certification, employees may spot check people from minority ethnic groups far more than white people. While they may ultimately gain access to the setting, the experience of feeling singled out could still cause distress, a loss of time, distrust in the scheme, and anxiety about future use. Concerns regarding discrimination are apparent in public polling: minority ethnic people report 18% more concern than White respondents that they would be discriminated against through vaccine passports, and 54% of all surveyed people think it is likely that vaccine passports would lead to discrimination against marginalised groups.[38]
Religion or belief
Background
Attending a place of worship is for many an important role in promoting their spiritual wellbeing and mental health, as well as contributing to a reduction in social isolation and loneliness.
Limitations on attending places of worship (including closure of in person worship) has impacted on people's ability to practice certain aspects of their faith, such as to congregate for worship in line with their Article 9 rights under the European Convention on Human Rights (freedom of religion).
Differential impacts
Positive impacts
There is an exception within the regulation for certain purposes, including worship, un-ticketed events held at an outdoor public place with no fixed entry points and certain business events that individuals are required to attend for work purposes. Certification would therefore not impact on freedom of religion (Article 9).
Negative impacts
People of certain religions may choose not to be vaccinated because it goes (or is perceived to go) against their beliefs. Examples include Muslim or Jewish people if a vaccine contains, or is believed to contain, pork cells, or Orthodox people if a vaccine contains, or is perceived to contain, embryonic cells. An interfaith statement, which urged people to come forward for vaccination, was issued by faith leaders.[77] The Muslim Council also issued a statement encouraging people to be vaccinated[78] and ran a vaccination campaign.[79]
There are also other beliefs and convictions, such as veganism[80], which may result in a person choosing not to be vaccinated, as it has been tested on animals. Therefore if people choose not to be vaccinated because of a belief then they may be negatively impacted by Certification if they are not able to gain entry to a regulated setting.
Sex
Background
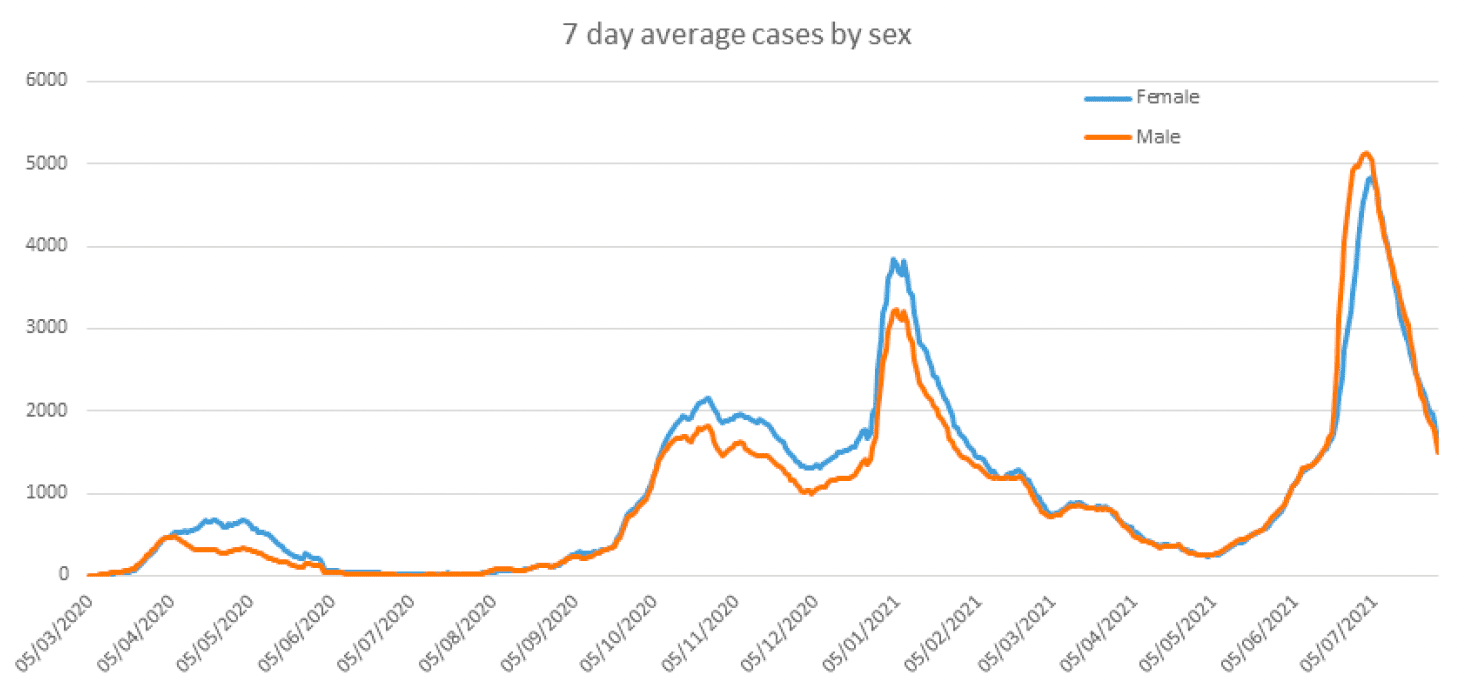
As can be seen in Figure 2, more women tested positive than men during lockdown periods (March-June 2020, December-March 2020-21). This is partly due to the fact that women are more likely to work as a key workers and in people-facing roles that carry greater risk of infection.
Figure 2: Women and men testing positive for Covid during lockdown periods (March-June 2020, December-March 2020-21).
Source: Public Health Scotland
Despite testing positive more often than men, data from up to September 2020 showed that, after adjusting for age, males were 1.4 times more likely to die than females.[81] However, there is emerging evidence that women may be more affected by long Covid.[82]
Scottish research into mental health impacts during the first wave of the pandemic shows that women reported higher levels of psychological distress than men across all ages, as well as symptoms of depression and anxiety.[14] This is consistent with UK-wide research on the mental health gender gap which, looking at data from the first wave, found that having a larger social network before the pandemic was strongly associated with larger declines in well-being after the onset of the pandemic: women reported more close friends before the pandemic than men, and higher loneliness than men after the pandemic started.[83]
The pandemic has increased socio-economic inequalities for women and they are overly represented in many 'shut down' sectors, such as retail, accommodation and food and beverage service activities.[84]
Domestic abuse is highly gendered: in the period 2018/20 16.5% of adults had experienced at least one incident of partner abuse since the age of 16; higher in women (21.2%) than men (11.2%).[85] Out of the 60,641 incidents police recorded in 2018-19, four of every five incidents where gender had been recorded had a female victim and a male accused.[86] Throughout the pandemic rates of domestic abuse have increased: the domestic abuse and forced marriage helpline received 95% more calls in the period April-June 2020 than in the same period the previous year, and a 27% increase for the 2020-2021 year overall compared to the previous.
Differential impacts
Positive impacts
If the policy objectives to reduce the risk of transmission and to increase vaccine uptake are achieved, Certification could positively impact men, as they are at a slightly higher risk of poorer health outcomes if they contract the virus.
British data from 2015 suggests that, although men spend on average more time than women on leisure activities in general, women spend on average more time socialising.[87] Therefore if the policy objective of allowing higher risk settings to continue to operate as an alternative to closure or more restrictive measures is achieved, Certification could benefit women as it facilitates their ability to socialise.
As previously stated, public insights polling found that women were 7 percentage points more likely than men (women 65% vs men 58%) to agree that, it they wanted to go to premises or an event, having a Covid Vaccine Certification scheme in place would make them feel more comfortable doing this.[88] Certification could add a layer of reassurance to women and support them to feel safer and more confident participating in society.
Additionally, stakeholders stated that any measure that avoids future restrictions or closure would be welcomed by women in abusive relationships, who have suffered disproportionately during lockdowns, and by women more generally, who are more likely to be working in the sectors that Certification may allow to remain open.
Negative Impacts
A study that uses the UK Household Longitudinal Study, a nationally representative panel, found 21% of surveyed women indicated vaccine hesitancy compared to 14.7% of men, with women estimated to be around 1.55 times more likely to be vaccine hesitant than men. The study also highlights that women were more likely than men to state that their main reason for vaccine hesitancy was concern about side effects, and that they do not trust vaccines.[89] Therefore, as women are more likely to be vaccine hesitant, they may be more likely to be denied access to a setting in scope due to not having a vaccine certificate.
Studies have found that facial recognition software has gendered and racial bias and "generally work best on middle-aged white men's faces, and not so well for people of colour, women, children, or the elderly".[90] Therefore when registering for the App it is possible that a slightly higher proportion of women may not be able to have their identity automatically verified.
Stakeholders informed us that women are more likely to share their phones with family members, such as their children. As the App can only log into one person's profile at time, women may be more likely to apply for a paper Certification for themselves or family members.
There is the possibility that Certification could be used beyond the intended purposes by private businesses and third parties as a condition of employment. As women are more likely to be vaccine hesitant than men and less likely to have Certification, this would likely impact women more than men. The pandemic has already exacerbated socio-economic and workplace inequalities for women, so if the policy intention was exceeded there is the possibility this could be aggravated.
Finally, as with older or disabled people, there is the risk that Certification could be used as a tool to enact coercive control. This would likely impact women far more than men as evidence shows domestic abuse is highly gendered.
Sexual Orientation
Background
In 2018, 2% of people in Scotland identified as lesbian, gay, or bisexual (LGB).[91]
During the pandemic, loneliness and isolation has strongly impacted LGB people of all ages. A survey of 2,934 secondary school pupils (1,140 of whom identified as LGBT+) by Just Like Us found that LGBT+ young people are twice as likely as their non-LGBT peers (52% vs 27%) to have felt lonely and separated from the people they are closest to on a daily basis during lockdown. 68% of LGBT+ young people survey also reported their mental health has worsened since the pandemic began, compared with half (49%) of non-LGBT+ young people.[92] Age UK also reported that older LGBT people are especially at risk of loneliness, as they are more likely to be single, live alone, and have less contact with relatives.[93]
While data from 2019 suggests that only 0.3% more men in the UK contracted HIV through sex with other men than with women,[94] HIV still has a strong historical and cultural connection with the LGB community. A study from England in December 2020 showed that the risk of dying from Covid-19 for people with HIV was more than double that of the rest of the population, even after adjusting for factors such as deprivation, ethnicity, smoking and obesity.[95] However, a note in the Lancet stated that, while clinicians should treat the findings as important, conclusions should be taken with caution until we have more specific controlled data to assess the effects of HIV on Covid-19 outcomes.[96]
Differential impacts
Positive impacts
If the policy objectives to reduce the risk of transmission and to increase vaccine uptake are achieved, Certification could positively impact people living with HIV, as they are at a higher risk of poorer health outcomes if they contract the virus. It may also support them to feel safer and more confident participating in society if they know that those around them have been vaccinated.
If the policy objective of allowing higher risk settings to continue to operate as an alternative to closure or more restrictive measures is achieved, Certification could positively impact LGBQ+ people as it facilitates their ability to socialise. This is particularly important for older people within the gay community who report higher rates of loneliness.[93]
Negative impacts
Despite their higher risk of death from Covid-19, stakeholders have informed us that some HIV positive people feel hesitant about the vaccine due to fears about side effects and that it may interact poorly with their HIV medication.[9798] Therefore, if HIV positive people are less likely to be vaccinated, Certification could have a negative impact if they are denied access to the settings in scope.
As detailed in the Gender Reassignment section, LGBT people are less likely to have ID than the general population, and so they may be slightly more likely to face difficulties registering for the App and more likely to use the paper Certificate.
Mitigating actions
The Scottish Government consider that, subject to the below mitigations being implemented, where Certification does engage rights, it does so in a proportionate way in order to protect public health.
Recognising not everyone has or can be vaccinated
Inclusive vaccination programme: to maximise uptake, there will be continued focus on the Inclusive Vaccine Programme, which includes targeted outreach and tailored communications e.g. Public Health Scotland and third sector partners have ensured the provision of a range of translated materials, British Sign Language (BSL) versions and other resources, such as the Covid-19 vaccine NHS Scotland explainer video, to ensure that everyone is able to access this information. More information on the Inclusive Vaccination Programme and the National Inclusive Steering Group for Covid-19 Vaccinations can be found online.
Exemptions: there are limited circumstances where a person may not yet have been vaccinated or may not be able to be vaccinated for legitimate reasons. For this reason, there are exemptions in the regulations for under 18s those with certain medical conditions, and those participating in vaccine trials. Medical exemptions may be available in a future iteration of the domestic App so that medical data is not shown when a staff member scans an exempt person's Certification.
Testing: initially, the scheme will not permit a negative test result to be offered as an alternative to evidence of vaccination, but this will be kept under review. At this stage, we do not consider that this would be appropriate and, indeed, could undermine one of the policy aims of the scheme, which is to increase vaccine uptake. Also, it is important at this stage to prioritise PCR lab capacity for Test and Protect purposes and while promoting regular LFD tests is an extremely important aspect of our overall approach, further work would be required on an optimal approach to incorporating testing, including consideration of the appropriateness of self-testing in this context.
Increasing accessibility
Paper Certification: in order to ensure Certification is accessible to all and to mitigate against digital exclusion, which is higher among older people, disabled people and some minority ethnic groups. We are translating documents that explain what is shown on your Certificate into different languages and formats, including Easy Read, audio and Braille.
The Covid-19 Status Helpline: to ensure that those who do not have digital access have a route to request their vaccination record. The helpline will also be available for people who cannot verify their identity on the App. The Covid-19 Status Helpline is free and open every day from 10:00-18:00.
A Resolver Group: has been established by NHS National Services Scotland to resolve any reported inaccuracies in vaccination records and wider issues relating to acquiring Covid Vaccine Certificate. Any requests for support can be escalated through the Covid-19 Status Helpline.
Communications and marketing: the implementation of Certification will be supported by a range of communications and marketing resources and activity to help people understand where the scheme has been introduced, for what purpose and how to gain certification. This will provide information about identifying and avoiding scams and phishing attempts, and will take the opportunity to reinforce messaging that vaccination data will not be shared with the Home Office or impact on immigration status, unless shared by the data subject themselves (e.g. when they go on holiday) or in exceptional circumstances when required by law. It will also provide information on and raise awareness of schemes like the Proof of Age Standards Scheme (PASS) and the Young Scot National Entitlement card.
Data protection and privacy
Data Protection Impact Assessment (DPIA) and Privacy Notice (PN): these are created to ensure that all data is managed, handled, processed and destroyed in line with UK GDPR legislation, data protection laws and data ethics best practice as well as human rights legislation. The PN will support users to understand how their data is being used throughout these processes, emphasising protection of their data and ensuring government is being open and transparent. The Privacy Notice is already online and can be found on NHS Inform: Personal information we process, How we use your data, Your Rights. The Easy Read Version can be found online.
Domestic App: is being developed and will be available by mid-October. This will show less data than the international Certificate which will mitigate against disproportionally engaging an individual's right to privacy (Article 8 right to respect for private and family life). The domestic App will have functionality to hide and display a person's name. Individuals can create separate profiles for international and domestic use using different email addresses. If an individual wishes to use a different name domestically, and has photo ID in that name, they can create one account for international travel, which aligns with the details on their passport, and one account for domestic use, which aligns with their preferred name.
ID Verification: Jumio, the company providing the software, state that their software has equal rates of success across all demographics with a matching rate of over 95%. For the other 5% there will be a manual check by Jumio staff to verify the user's identity.
Supporting implementation in line with our policy aims
Sectoral guidance: to support effective implementation consistent with our policy aim, we have provided information to the sectors where Certification is mandated on the policy and regulations, and the appropriate implementation, enforcement and handling of exemptions. This guidance can be found on the Scottish Government website.
Ministers have been clear that certification will not be a requirement for public services or other settings that many people have no option but to attend such as retail, public transport, health services and education. We recognise that some businesses, outside the regulated settings, are asking people for evidence they have been fully vaccinated as a condition of entry or as a condition of employment. We emphasised in our guidance that businesses which are not covered by the Government's scheme would need to consider carefully their approach, in accordance with obligations under all relevant laws including data protection, the Equality Act and Human rights. For more information see the Equality and Human Rights Commission Guidance for Employers.
Enforcement of regulations from 18 October: we have listened to businesses carefully and, as such, after the scheme comes into force at 5 am on Friday 1 October, we will allow a period of slightly more than two weeks – until 18 October – before the requirement to have a reasonable system in operation for checking Certification becomes enforceable. This period – effectively a grace period – will allow businesses to test, adapt and build confidence in the practical arrangements they will have to introduce to comply.
Public guidance: we will also produce guidance for the wider public to provide information on what Certification is, the policy objectives, where it is regulated and why, and the steps to attain Certification. Our Guidance will be clear about the settings in which use of Certification is appropriate to mitigate the risk that businesses and other entities consider using Certification in relation to activities and services which fall outside the regulations. It will explain that the scope of the Regulations has been carefully and deliberately limited to activities where the balance of public health risk clearly outweighs other rights considerations, and is designed to respect the rights of individuals. Specific protections, applicable within the limits of the statutory scheme, have been put in place to ensure the scheme operates in a lawful manner.
Ongoing stakeholder engagement: We will continue to engage with stakeholders and gather intelligence on the impact of Certification. We will create feedback loops and build this evidence into the policy.
Exceptions: There will be exceptions for premises being used for certain purposes, including worship, un-ticketed events held at an outdoor public place with no fixed entry points and certain business events that individuals are required to attend for work purposes.
Monitoring and evaluation
Any policy that engages human rights needs to meet the test of necessity and proportionality at any given time, and should be immediately removed if it is found to no longer meet that test.
The Scottish Government will be responsible for monitoring and evaluating the policy. As the regulations have been laid under the Coronavirus Act 2020 there is a requirement to review the regulations every 21 days. The extent to which the policy (Covid Vaccine Certification) is achieving the policy objectives (reduce the risk of transmission of Coronavirus, reduce the risk of serious illness and death thereby alleviating current and future pressure on the National Health Service, allow higher risk settings to continue to operate as an alternative to closure or more restrictive measures and increase vaccine uptake) will be monitored and evaluated in line with this requirement. Monitoring and evaluation will also provide us with further information about other positive and negative effects of the introduction of the policy. We will also continue to assess whether any less intrusive measures could be introduced to achieve the same combination of policy objectives in respect of the higher risk sectors concerned; if so, the policy will be immediately reviewed.
The Covid Vaccine Certificate provisions will expire on 28 February 2022, as with all other Covid measures under the Health Protection (Coronavirus) (Requirements) (Scotland) Regulations 2021. Parliamentary approval would be required to extend them further.
To that aim, we will continue to consider the impact of Certification on protect characteristics and our obligations under the public sector equality duty. This will include engaging with relevant stakeholders and we will publish further equality impact assessments (EQIA) if needed.
Contact
There is a problem
Thanks for your feedback